
Adjustment Disorder with Mixed Disturbance of Emotions and Conduct (AD-MDEC) shows up as both emotional turmoil and behavioral shifts for clients. Common symptoms can be irritability, sadness, impulsivity, or acting out under stress.
In this guide, we’ll walk through evidence-based treatments like CBT, DBT, family therapy, and holistic interventions — plus how you can set goals, build treatment plans, and track progress over time for your clients.
For therapists who want to save time without compromising care quality, Mentalyc’s AI Treatment Plan Generator can automatically turn your session insights into measurable, compliant treatment plans that stay aligned with each client’s evolving needs.
Understanding Adjustment Disorder with Mixed Disturbance of Emotions and Conduct
Adjustment Disorder with Mixed Disturbance of Emotions and Conduct (AD-MDEC) is a stress-response condition that develops after a major life change or identifiable stressor, such as a breakup, job loss, or relocation. Clients often experience both emotional symptoms (like sadness, irritability, or anxiety) and behavioral changes (such as impulsivity, aggression, or withdrawal).
Automated treatment plans that reflect your approach

New! Transfer your notes to EHR with a single click. No more copy-pasting.
Because these reactions arise from the way individuals process and adapt to stress, treatment must address the connection between emotions, thoughts, and behaviors. This is where psychotherapy for adjustment disorder (“talk therapy”) plays a central role.
Depending on the presentation, therapists may use therapy for adjustment disorder such as Cognitive Behavioral Therapy (CBT), Dialectical Behavior Therapy (DBT), Family Therapy, or Trauma-Focused approaches to guide recovery.
Evidence-Based Treatments for Adjustment Disorder with Mixed Disturbance of Emotions and Conduct
| Therapy Type | Primary Focus | Key Techniques | Best For | Expected Outcomes |
| Cognitive Behavioral Therapy (CBT) | Identifying and changing maladaptive thoughts and behaviors | Cognitive restructuring, behavioral activation, problem-solving | Clients with negative thinking patterns, low mood, or avoidance behaviors | Improved coping skills, reduced depressive and anxious symptoms |
| Dialectical Behavior Therapy (DBT) | Emotion regulation and impulsivity management | Mindfulness, distress tolerance, emotion regulation, interpersonal effectiveness | Clients with emotional dysregulation, anger, or impulsive conduct | Better emotion control, reduced self-destructive or impulsive behaviors |
| Family Therapy | Strengthening family communication and support | Boundary setting, conflict resolution, psychoeducation | Children, adolescents, or adults with family-related stressors | Healthier family dynamics, increased emotional support |
| Trauma-Focused Therapy (TFT) | Processing trauma linked to stressor events | Narrative therapy, EMDR, grounding techniques | Clients whose AD-MDEC is triggered by trauma or loss | Reduced intrusive thoughts, better emotional integration |
| Mindfulness-Based Therapy | Promoting present-moment awareness and stress reduction | Guided meditation, body scans, breathwork | Clients with anxiety, tension, or poor stress tolerance | Improved self-regulation, lower physiological arousal |
| Behavioral Interventions | Replacing maladaptive behaviors with adaptive ones | Behavior contracts, reinforcement plans, role-play | Children or adults with conduct issues, aggression, or defiance | Increased prosocial behavior, decreased acting-out behaviors |
1. Cognitive Behavioral Therapy for Adjustment Disorder
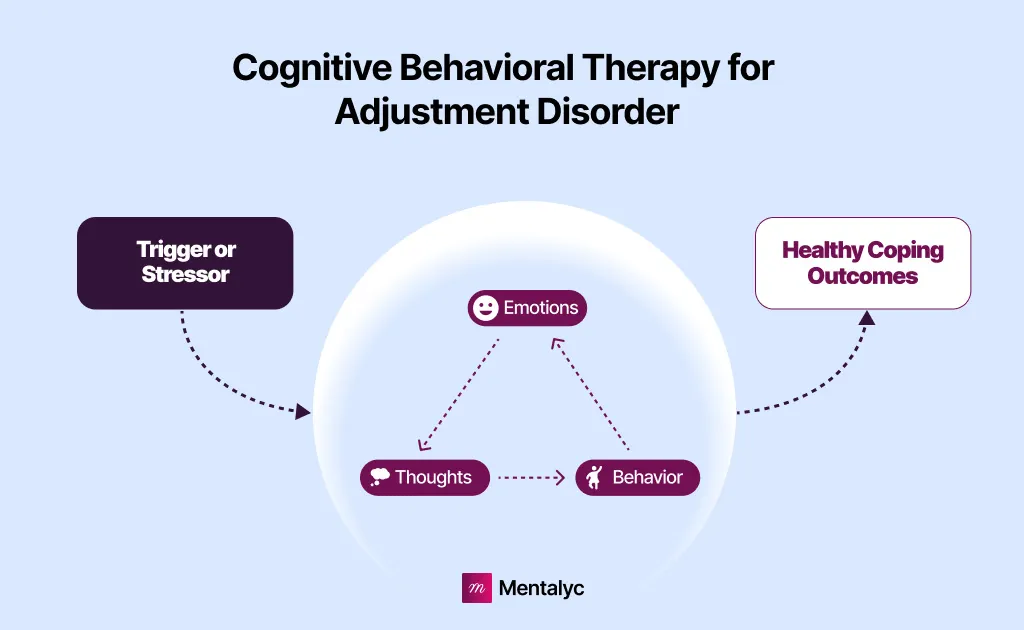
Cognitive Behavioral Therapy (CBT) is highly effective for addressing the emotional and behavioral components of AD-MDEC. It helps clients identify and challenge maladaptive thoughts, develop healthier coping mechanisms, and regulate emotions.
CBT Techniques:
- Cognitive Restructuring: Helps clients challenge negative thoughts such as “I’ll never recover from this loss” or “I can’t control myself!”
- Behavioral Activation: Encourages engagement in meaningful activities to reduce depressive symptoms.
- Problem-Solving Skills Training: Teaches clients how to manage stressors effectively.
- Role-Play: Prepares clients for real-life situations, such as handling conflict without aggression.
Clinical Example of CBT:
A 17-year-old client experiencing school failure after her parent’s divorce exhibits defiance at home. She is sad and lonely and has started vaping.
CBT sessions focus on identifying irrational beliefs (e.g., “I’m worthless because I caused my parents’ divorce!”), developing alternative perspectives (e.g., “This is a tough time, but I can still do well in school”), and setting small, achievable goals to rebuild confidence (e.g., “I’m going to join a support group with other teens to build connections and eventually stop relying on my vape.”).
2. Dialectical Behavior Therapy (DBT) for Emotional Dysregulation
**Dialectical Behavior Therapy, or DBT for adjustment disorder** is beneficial for clients with emotional dysregulation and impulsive behaviors.
DBT Techniques:
- Mindfulness: Encourages clients to observe their thoughts and emotions without judgment.
- Distress Tolerance: Teaches strategies for managing crises, such as deep breathing and grounding exercises.
- Emotion Regulation: Helps clients understand and manage intense emotions.
- Interpersonal Effectiveness: Develops assertive communication skills to manage conflicts.
Clinical Example:
A 29-year-old client struggling with anger and impulsivity after losing his job learns distress tolerance techniques like TIP (Temperature, Intense exercise, Paced breathing) to manage his rage during arguments.
3. Family Therapy for Adjustment Disorder
Family therapy is essential, especially for children and adolescents, as family dynamics often contribute to stress or maintain the symptoms.
Family Therapy Goals:
- Improve communication patterns within the family.
- Create a supportive environment for the client.
- Address parental or sibling dynamics contributing to behavioral issues.
Clinical Example:
In family therapy, parents of a 16-year-old learn to set consistent boundaries while validating the teen’s emotions. The family also collaboratively identifies stress-reducing strategies.
Automate Treatment planning with Mentalyc’s AI Treatment Planner
Generate treatment plans that mirror your approach, satisfy payors, and evolve with your clients.
- SMART Goals
- Insurance-ready formatting
- Track goals & outcomes
- HIPAA & PHIPA compliant
New! Transfer your notes to EHR with a single click. No more copy-pasting.
4. Trauma-Focused Therapy and EMDR
Trauma-Focused Therapy (TFT). If a traumatic event triggers AD-MDEC, trauma-focused therapy can help clients process the experience and reduce symptoms.
TFT Techniques:
- **Narrative Therapy:** Helps clients construct a coherent story about the stressor, reducing its emotional impact.
- Eye Movement Desensitization and Reprocessing (EMDR): Reduces distress related to traumatic memories.
Clinical Example:
A 21-year-old client who developed AD-MDEC after surviving a natural disaster works with his therapist to reprocess traumatic memories using EMDR for trauma-related adjustment disorder, helping him reduce intrusive thoughts, nightmares, and emotional reactivity.
Psychoeducation and Behavioral Interventions
Psychoeducation in Therapy
Psychoeducation is the foundation of treatment, helping clients and their families understand the nature of AD-MDEC and how it affects emotions and behavior.
Focus Areas:
- The link between stressors, emotions, and behavior.
- Recognizing triggers and early warning signs of distress.
- Developing healthy coping mechanisms.
Example: Parents of a 9-year-old learn to differentiate between intentional misbehavior and stress-related acting out, enabling them to respond more effectively.
Behavioral Interventions for Emotional Disturbance
Behavioral Interventions. Targeted behavioral interventions can help reduce problematic behaviors for clients with significant conduct-related symptoms.
Behavior management plans are particularly effective for children and adolescents, as the plans establish clear expectations, rewards for positive behavior, and consequences for negative behavior.
Steps:
- Identify target behaviors (e.g., physical aggression, defiance).
- Develop a reward system for desired behaviors.
- Implement consistent consequences for problematic behaviors.
Example: A teacher collaborates with a therapist to create a reward chart for a 10-year-old student with AD-MDEC. The student earns points for completing assignments and using conflict resolution skills, which can be exchanged for privileges like extra recess time.
Clients often struggle with interpersonal interactions, leading to social withdrawal or conflict. Social skills training teaches appropriate ways to communicate and resolve disputes.
Skills Taught:
- Active listening.
- Assertive communication.
- Conflict resolution.
Example: A 34-year-old client with difficulty making friends due to aggressive outbursts practices introducing themselves and responding calmly to disagreements during role-play sessions.
Medication and Pharmacotherapy Options
| Medication Class | Examples | Primary Purpose | When It’s Used | Key Considerations |
| Selective Serotonin Reuptake Inhibitors (SSRIs) | Sertraline (Zoloft), Fluoxetine (Prozac), Escitalopram (Lexapro) | Reduce depressive and anxiety symptoms | When clients show persistent sadness, irritability, or worry | Start with low doses; monitor for side effects and gradual improvement |
| Mood Stabilizers | Lamotrigine (Lamictal), Valproate (Depakote) | Control mood swings and irritability | When clients have emotional instability or impulsivity | Regular monitoring needed for dosage and side effects |
| Stimulants / Non-Stimulants (for comorbid ADHD) | Methylphenidate (Ritalin), Atomoxetine (Strattera) | Enhance focus and reduce impulsivity | For clients with concurrent ADHD or attention issues | Should be prescribed alongside therapy and close monitoring |
Pharmacotherapy. While psychotherapy is the cornerstone of treatment, pharmacotherapy for adjustment disorder can be considered for clients with severe symptoms or co-occurring disorders.


Medication Options:
- Selective Serotonin Reuptake Inhibitors (SSRIs): For clients with significant anxiety or depression (e.g., sertraline, fluoxetine).
- Mood Stabilizers: For clients with severe emotional dysregulation (e.g., lamotrigine).
- Stimulants or Non-Stimulants: For clients with concurrent ADHD and behavioral symptoms (e.g., methylphenidate, atomoxetine).
Example: A 19-year-old client with AD-MDEC and comorbid major depressive disorder benefits from fluoxetine, which reduces depressive symptoms and enhances the effectiveness of CBT.
Mind-Body and Holistic Approaches
Holistic treatment for adjustment disorder can complement traditional therapies, addressing the physiological aspects of emotional and behavioral dysregulation.
- Mindfulness and Meditation. Mindfulness practices help clients stay present and manage emotional reactivity.
- Physical Activity. Exercise has well-documented benefits for reducing stress, improving mood, and enhancing self-regulation.
- Art and Music Therapy. Creative therapies can provide a safe space for clients to express emotions and process experiences.
Building a Support System for Recovery
Establishing a Support System. Social support plays a critical role in recovery. Clients are encouraged to strengthen existing relationships and build new connections.
Strategies:
- Join support groups or community activities.
- Strengthen family or friend relationships through shared activities.
- Reduce isolation by volunteering or engaging in hobbies.
Example: A 50-year-old client joins a local hiking club, helping her build a sense of community and reduce loneliness.
Stressor-Specific Interventions
Stressor-Specific Interventions. Since AD-MDEC is triggered by identifiable stressors, addressing the root cause is essential.
Examples of Stressor-Specific Interventions:
- Work-Related Stress: Career counseling or time management training.
- Relationship Conflicts: Couple’s therapy or communication skills training.
Example: A 39-year-old client overwhelmed by recent relocation benefits from problem-solving sessions to develop a plan for settling into his new environment, such as finding social opportunities and organizing his new home.
Creating an Individualized Treatment Plan for AD-MDEC
Each client’s treatment plan should address emotional, behavioral, and environmental factors contributing to their symptoms.
For therapists who spend hours building and updating treatment plans, Mentalyc helps you transform notes into smart treatment plans that stay clinically accurate and easy to update.
Here’s an example of treatment plan for adjustment disorder:
Treatment Plan Example: Maria, 28 Years Old
- Client: Maria, 28-year-old woman.
- Stressors: Job loss and breakup.
- Symptoms: Depression, irritability, avoidance of social contact, impulsive spending.
Initial Assessment
- Evaluate emotional symptoms such as anxiety, depression, and irritability.
- Assess behavioral symptoms, including aggression, impulsivity, and avoidance.
- Identify the stressors (job loss and breakup) and their impact on Maria’s emotional and behavioral state.
- Screen for co-occurring disorders, such as substance use or anxiety disorders that may influence Maria’s symptoms.
Short-Term and Long-Term Treatment Goals for AD-MDEC
| Time Frame | Treatment Goals | Therapeutic Focus | Example Interventions | Expected Outcomes |
| Short-Term (0–4 weeks) | Stabilize acute symptoms such as irritability, impulsive spending, and anxiety | Psychoeducation for client and family; emotional stabilization | Provide education about AD-MDEC and stressor impact; introduce grounding or relaxation techniques; identify early triggers | Reduced impulsivity and anxiety; improved understanding of disorder and stress responses |
| Mid-Term (1–3 months) | Develop adaptive coping and cognitive restructuring skills | Replace maladaptive behaviors; improve problem-solving and self-esteem | Implement mindfulness and behavioral activation routines; use CBT to reframe negative thoughts; practice budgeting and daily structure | Improved mood and self-efficacy; healthier coping patterns; reduced financial or relational stress |
| Long-Term (3–6 months+) | Build resilience and emotional self-regulation | Strengthen social support and prevent relapse | Continue CBT or DBT sessions; encourage social reconnection with family and peers; reinforce emotional regulation techniques | Sustained emotional balance, stronger relationships, and long-term behavioral stability |
Expected Outcomes and Long-Term Recovery
Goal 1: Stabilize Maria’s acute emotional and behavioral symptoms.
- Objective: Reduce depressive symptoms and impulsivity.
- Intervention: Introduce a low-dose SSRI to alleviate persistent depressive symptoms under psychiatric care.
Goal 2: Increase Maria’s understanding of her condition and enhance family support.
- Objective: Provide psychoeducation on AD-MDEC and its connection to her symptoms.
- Intervention: Conduct a family session with Maria and her sister to discuss the disorder and their roles in the treatment process.
Goal 3: Replace maladaptive behaviors with adaptive coping mechanisms.
- Objective: Develop a daily schedule of purposeful activities to rebuild routine.
- Intervention: Implement Behavioral Activation by scheduling structured activities, such as applying for jobs, exercising, and engaging in hobbies.
Goal 4: Address maladaptive thought patterns and strengthen problem-solving skills.
- Objective: Reframe Maria’s negative beliefs about her self-worth and financial situation.
- Intervention: Use CBT techniques such as cognitive restructuring and thought-tracking to challenge and change maladaptive thoughts.
Goal 5: Build resilience and emotional regulation skills for long-term stability.
- Objective: Teach grounding and mindfulness techniques for anxiety management.
- Intervention: Introduce mindfulness exercises, such as guided breathing and body scans, to enhance emotional self-regulation.
Summary of Interventions
- Cognitive Behavioral Therapy (CBT): Address maladaptive thought patterns and strengthen coping strategies.
- Behavioral Activation: Rebuild Maria’s routine and purpose through structured activities.
- Family Involvement: Engage Maria’s sister to provide support, accountability, and encouragement.
- Mindfulness Practice: Introduce grounding techniques and mindfulness exercises for anxiety and emotional regulation.
- Medication Management: Prescribe and monitor a low-dose SSRI for depressive symptoms.
Expected Outcomes
Within three months, Maria will demonstrate:
- Stabilized emotional symptoms, such as reduced irritability and improved mood.
- A consistent daily routine, including job applications and social engagement.
- Enhanced coping skills and resilience, reducing impulsivity and anxiety.
- Secured new employment and reestablished a sense of purpose
Conclusion: Empowering Clients Toward Emotional Stability
Adjustment Disorder with Mixed Disturbance of Emotions and Conduct requires a thoughtful, individualized approach that addresses emotional and behavioral symptoms. By combining evidence-based treatments like CBT, DBT, family therapy, and stressor-specific interventions, therapists empower clients to regain stability and increase resilience. Collaboration with clients and their support systems fosters long-term recovery and prevents relapse.
For therapists who want to make treatment planning more efficient and data-informed, Mentalyc offers smart treatment plans – ****turning session notes into structured goals and measurable outcomes, so you can focus more on healing and less on documentation.
FAQs About Treatment for Adjustment Disorder with Mixed Disturbance of Emotions and Conduct
What is Adjustment Disorder?
Adjustment Disorder is a stress-related mental health condition that occurs when a person struggles to cope with a major life change or event. It leads to emotional and behavioral symptoms—such as sadness, anxiety, or irritability—that interfere with daily functioning but are not as severe as major depressive or anxiety disorders.
How is Adjustment Disorder with Mixed Disturbance of Emotions and Conduct treated?
Treatment for Adjustment Disorder with Mixed Disturbance of Emotions and Conduct (AD-MDEC) combines psychotherapy, such as CBT or DBT, with behavioral interventions, family therapy, and sometimes pharmacotherapy. The goal is to reduce emotional distress, manage impulsive behaviors, and help clients build healthier coping and problem-solving skills.
What is the best therapy for Adjustment Disorder?
The best therapy for Adjustment Disorder will depend case by case. But the most common therapy for Adjustment Disorder is Cognitive Behavioral Therapy (CBT). CBT helps clients identify negative thought patterns, reframe stress responses, and adopt adaptive coping strategies. Therapists may also integrate DBT or family therapy depending on the client’s symptoms and support system.
What are the treatment goals for Adjustment Disorder with Disturbance of Conduct?
Treatment goals focus on reducing aggression, impulsivity, and oppositional behaviors while improving emotional regulation and problem-solving. Therapists aim to build coping skills, strengthen family support, and restore functioning in social, academic, or work settings. Structured behavior plans and CBT-based interventions are typically used.
What is the gold standard treatment for Adjustment Disorder?
The gold standard treatment for Adjustment Disorder is psychotherapy, particularly Cognitive Behavioral Therapy (CBT). It is often supported by psychoeducation, family involvement, and mindfulness-based strategies. Medication may be added if symptoms of depression or anxiety significantly impair functioning.
What exercises are good for Adjustment Disorder?
Mind-body exercises like mindfulness meditation, yoga, and aerobic activity (such as walking or swimming) help lower stress and improve emotional regulation. Creative outlets like art or music therapy can also promote relaxation and emotional expression, complementing traditional therapy for Adjustment Disorder.
What are the DSM-5 criteria for Adjustment Disorder?
According to the DSM-5, Adjustment Disorder involves:
- Emotional or behavioral symptoms in response to an identifiable stressor within three months of onset.
- Distress that is out of proportion to the stressor.
- Impaired social, occupational, or academic functioning.
- Symptoms do not persist beyond six months after the stressor resolves.
References
American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders-TR (5th ed., Text Revision).
Beck, J. S. (2011). Cognitive Behavior Therapy: Basics and Beyond. Guilford Press.
Linehan, M. M. (2014). DBT Skills Training Manual (2nd ed.). Guilford Press.
Shear, K., & Ghesquiere, A. (2013). Adjustment Disorders: The Clinical Handbook. Journal of Clinical Psychology, 69(11), 1081-1082.
Sharf, R. S. (2016). Theories of Psychotherapy and Counseling: Concepts and Cases (6th ed.). Cengage Learning.
Why other mental health professionals love Mentalyc

“Do yourself a favor, make your life easier. I found Mentalyc to be one of the best tools that I’ve ever used.”
Licensed Marriage and Family Therapist

“If I were recommending this software to a colleague, I would tell them that it is the best thing that they could do for their practice.”
Licensed Professional Counselor

“For anyone hesitant: this is a lifesaver. It will change your life, and you have more time to be present with your patients.”
Licensed Clinical Social Worker

“It immediately changed my quality of life, personally and professionally.”
Owner/Independently Licensed Marriage & Family Therapist (LMFT)


