This guide gives therapists 15 ready-to-use progress note templates with full worked examples, plus the rules that keep notes audit-ready, HIPAA-compliant, and useful at the next session. Whether you run a solo private practice, work in a group practice, or supervise a team, the same templates apply.
There is no single “best” template. Many insurance companies require you to state what interventions you used and why the client needs therapy, otherwise known as medical necessity. The template you choose just needs to make that case quickly and consistently. When notes are connected to tools like Mentalyc’s AI Treatment Planner, aligning interventions with measurable goals takes minutes instead of hours.
This page is the templates and examples sub-pillar of our broader therapy notes guide. If you need the high-level rules of clinical documentation, start there. If you need a template you can paste into your EHR today, you are in the right place.
What Are Progress Notes in Mental Health?
Progress notes are clinical records that document what happened in a therapy session: the date, length, content, interventions used, and the client’s progress toward treatment goals. They are part of the official client record, accessible to other treating providers and, with proper authorization, to insurers.
A progress note has to do three jobs. It has to let any clinician picking up the chart understand the client’s diagnosis and current presentation. It has to document the functional impairments that justify medical necessity and the interventions used to address them. And it has to show that treatment is working, or give a clear clinical rationale for continuing it.
In short, a progress note is medical documentation: session details, diagnosis, observations, interventions, and progress. Progress notes exist to show the course of improvement or decline to the clinician, third-party reviewers, and the client. Without them, a new provider picking up the case would have to start from scratch, wasting time and resources at the client’s expense.
Progress Notes vs. Psychotherapy Notes
Progress notes and psychotherapy notes are not the same record. Progress notes are part of the medical chart and can be shared with insurers and other providers. Psychotherapy notes (also called process or private notes) are the clinician’s personal observations, kept separate from the chart, and receive stronger HIPAA protection. See process notes vs. progress notes for the full distinction.
Progress Notes at a Glance (HIPAA-Aligned)
| Feature | Progress Notes |
|---|---|
| Purpose | Document the client’s presentation, diagnosis, treatment plan, and progress toward therapeutic goals. |
| Written and used by | All of the client’s healthcare providers, plus authorized third parties such as insurers. |
| Content | Presenting problems, medical history and diagnosis, prescriptions, treatment plan, symptom progress, other relevant information. |
| Style and structure | Concise, highly structured, formal, objective, clinical language. |
| Sharing and privacy | HIPAA-protected. Typically shared with other healthcare providers, third parties such as insurance companies, and the client on request. |
What to Include in Every Progress Note
Every progress note should answer the following questions:
- What is the current medical necessity for services?
- What was discussed in the session?
- What clinical observations were made?
- What therapeutic interventions and techniques were used, and how effective were they?
- What progress or setbacks occurred?
- Which signs and symptoms are still present, improved, worsened, or no longer present?
- How and how much are treatment plan goals being met?
- What are the client’s current limitations and strengths?
Alongside that clinical content, every note also needs the basic session metadata payers and auditors look for: start and stop times, location, date of service, client name plus a second unique identifier, and provider name and credentials. Tie each note to at least one treatment plan goal so medical necessity is visible at a glance.
A practical target length is 150 to 400 words per session. Long enough for another clinician to understand what happened and what comes next, short enough to actually finish. Best practice is to write or finalize each note within 24 to 48 hours of the session, while details are fresh and the chart stays audit-ready. CMS guidance recommends completing documentation no later than 72 hours after the visit.
How to Write Good Progress Notes
Five rules cover most of what makes a clinically useful, audit-ready note.
1. Be professional and to the point. Other healthcare providers will read these notes. Avoid heavy abbreviations and keep prose tight enough that someone picking up the chart can grasp the client’s history in under a minute.
2. Write objectively. Third person, no slang, no personal feelings about the client’s progress.
3. Back observations with evidence. If the client presents with a low mood, document the markers: affect, body language, self-report. Show your reasoning.
4. Get the metadata right. Date, time, location, diagnostic code, signature. These are the first things an auditor checks.
5. Use a template. SOAP, DAP, BIRP, GIRP, PIRP, PIE, or a custom format. Pick one that fits the session and stick with it across the episode of care.
Stop spending nights on progress notes

SOAP Note Template and Example for Mental Health Progress Notes
SOAP notes have four sections: Subjective, Objective, Assessment, Plan. SOAP is the most common progress note format in behavioral health because it maps cleanly to the medical model and satisfies most payer requirements.
Subjective. The client presents for therapy, wanting to work on symptoms associated with their Borderline Personality Disorder diagnosis. The client reports having trouble with interpersonal relationships and often feels like the people close to them will abandon them. The client says they struggle to relate to coworkers and maintain friendships. The client states they have had these problems throughout their life but noticed the relationship difficulties increasing in the last few months.
Objective. The client presents with a disheveled appearance. They are on time for the session and have a depressed presentation. The client appears in a low mood.
Assessment. The client appears to meet the Borderline Personality Disorder criteria. They have a history of challenges with maintaining friendships, which has increased in the last few months alongside increased stress.
Plan. The client will meet with the therapist weekly to work on symptoms associated with Borderline Personality Disorder. The therapist will utilize DBT techniques, such as helping the client learn interpersonal effectiveness skills. The therapist will also work toward helping the client identify a DBT group in the area they can join.
Mentalyc’s AI Note Taker drafts a SOAP note like this one in about two minutes from a session recording or upload. It is HIPAA-compliant, handles SOAP, DAP, BIRP, GIRP, PIRP, EMDR and 100+ other templates out of the box, and lets you tweak the structure to match your workflow without losing audit compliance.
For therapists who want deeper insight into session dynamics and the therapeutic alliance, Alliance Genie adds reflective analysis alongside the structured note.
SOAP Note Example: Follow-Up Session, Major Depressive Disorder
The example above is a typical first-session SOAP. Follow-up notes look slightly different. They are shorter, lean more on comparison to prior sessions, and update the treatment plan rather than establishing it.
Name: Tyler Kincaid · DOB: 10 December 1989 · Date of Session: 10 June 2026 · Time: 1:30 pm to 2:30 pm · Therapist: (Insert Name) · Session Type: Second (In-person)
S. Subjective. The client reported slight improvement in mood since the last session. He stated, “There have been a few good days in which I did things I liked.” He now gets out of bed earlier on most mornings. He continues to struggle with low energy but reported walking his dog three times in the past week. He still finds it difficult to eat enough. He denied any thoughts of suicide or self-harm. He said, “I couldn’t try out that coping skill you mentioned because it was hard for me.”
O. Objective. The client appeared less withdrawn than in the previous session. His mood seemed slightly improved. He maintained eye contact throughout the session. Speech was normal in tone and volume. He was neatly dressed in a blue shirt and brown khaki shorts. He showed signs of frustration when discussing the coping skill exercise. There were no visible signs of immediate distress.
A. Assessment. The client is a 35-year-old male presenting with symptoms of Major Depressive Disorder (MDD). He showed some progress in mood and activity level. He has begun re-engaging in daily tasks such as walking his dog. However, he was unable to apply the coping skill introduced in the last session. This area will need further support. He appears safe and stable at this time.
P. Plan.
- Explore the challenges he faced with using the coping skill.
- Break the mindfulness exercise into smaller, easier steps.
- Highlight and reinforce his recent progress, including walking his dog.
- Set one small, achievable goal for the new week, for example, complete one enjoyable activity daily.
- Schedule a follow-up session for 30 June 2026.
- Continue measuring progress and begin addressing cognitive distortions.
DAP Note Template and Example for Therapy Documentation
DAP notes have three sections: Data, Assessment, Plan. DAP merges SOAP’s Subjective and Objective into a single Data section, which makes it faster to write and well-suited to outpatient and community mental health settings. Here is a DAP note for a client with ADHD.
Data. The client presents for psychotherapy due to struggling to focus on his college classes. The client procrastinates and needs help completing homework by assigned deadlines. The client has consistently been late in turning in homework since the semester began. He also reports problems getting to class on time since the semester started three months ago.
Assessment. The client’s symptoms are consistent with ADHD. The counselor will work with him on strategies to help with task initiation as well as recognizing unhelpful thoughts that inhibit his ability to get his work done. The counselor will also speak with him about getting a formal assessment for ADHD and potential medication.
Plan. The client will meet with the counselor weekly to work on strategies for coping with ADHD. The counselor will give him an outside referral to a psychologist who does ADHD testing.
BIRP Note Template and Example for Behavioral Health Progress Notes
BIRP notes have four sections: Behavior, Intervention, Response, Plan. BIRP is best when the session is intervention-heavy and you want to clearly show what you did and how the client responded. Intensive outpatient programs frequently expect this format. Below is a BIRP note for trauma work.
Behavior. The client presents for therapy to work on challenges related to childhood trauma. The client reports flashbacks and nightmares regarding a sexual abuse incident in childhood. The client reports that these nightmares have affected sleep quality and are causing daytime fatigue.
Intervention. The counselor will utilize EMDR techniques to treat the client’s trauma. The counselor spent the first part of the session identifying coping skills and resources the client has used to process trauma and what has not helped.
Response. The client was on time for therapy and attentive. The client is receptive to starting EMDR, which will begin in the next session.
Plan. The client and counselor will start working on the first phase of EMDR in the next session. The counselor and client will meet weekly to work on the client’s past trauma.
BIRP Note Example: First Session, Trauma-Centered Therapy
The BIRP example above uses EMDR as the intervention. Trauma work does not always start there. Many first sessions focus on grounding, psychoeducation, and stabilization before any trauma-processing modality is introduced. Below is a BIRP note for that kind of first session.
Name: David Sheffield · DOB: 4 August 1979 · Date of Session: 18 June 2026 · Time: 11:00 am to 12:00 pm · Therapist: (Insert Name) · Session Type: First (In-person)
B. Behavior. The client reported an increase in flashbacks after watching a combat documentary. He described the experience as something that “brought back the dread.” He also reported poor sleep over the last three nights due to nightmares. He shared that he had avoided family and friends, saying he “couldn’t deal with people.” At the start of the session, he appeared quiet and tense.
I. Intervention. I validated the client’s trauma response and offered support. He was taught the 5-4-3-2-1 grounding technique to help reduce distress. We explored the connection between the documentary and his symptoms. I also explained how trauma can affect the body and mind. The session included education on reducing exposure to triggers and how to make use of available social support.
R. Response. The client was withdrawn at the beginning but became more engaged after practicing the grounding exercise. He reported feeling “a little bit present.” He identified specific media triggers and acknowledged that isolation had worsened his mood. He agreed to limit exposure to triggering content and to reach out to at least one supportive person. By the end of the session, he appeared more relaxed and said he felt more open.
P. Plan.
- Continue to monitor his trauma symptoms and how they affect his daily functioning.
- Reinforce the use of grounding techniques throughout the week.
- Discuss ways to improve and stabilize his sleep routine.
- Encourage avoidance of triggering media and increased use of support systems.
- Reschedule the next session for 29 June 2026. Focus will shift to understanding trauma responses and building additional relaxation skills.
Difference Between SOAP, DAP, and BIRP Notes
| Feature | SOAP Notes | DAP Notes | BIRP Notes |
|---|---|---|---|
| Full form | Subjective, Objective, Assessment, Plan | Data, Assessment, Plan | Behavior, Intervention, Response, Plan |
| Purpose | Detailed, medical-style documentation | Simplified format for mental health | Focuses on behavioral interventions and outcome |
| Best for | Medical and clinical settings | General therapy notes | Behavioral health and intervention tracking |
| Detail level | High | Moderate | Moderate |
| Used by | Therapists, psychiatrists, clinicians | Therapists, counselors | Behavioral therapists, social workers |
Which Progress Note Format Should You Use?
Match the format to the session and the payer.
- SOAP when you want a clean separation between client-reported and observed information. Default for most outpatient mental health work and the format most insurers recognize on sight.
- DAP when you want SOAP’s logic in a shorter shape. Good for brief sessions, case notes, and high-volume caseloads.
- BIRP when the session was intervention-heavy and you want to clearly show what you did and how the client responded. Common in IOPs and substance use programs.
- GIRP when documentation needs to map directly to a treatment plan goal. Often preferred by insurers for utilization review.
- PIRP when the session is organized around an identified problem, including crisis sessions and short-term work.
- PIE or custom when you need a lightweight structure or a specific section your payer asks for, such as risk assessment, strengths, or homework.
- SIRP (Situation, Intervention, Response, Plan) when documenting crisis or incident-driven sessions where the precipitating situation matters as much as the intervention.
- FIRP (Functioning, Intervention, Response, Plan) when functional impairment is the central organizing concept of the session, common in community mental health and rehabilitation settings.
- Narrative when the session is psychodynamic, humanistic, or integrative and reads more naturally as a session summary than as a structured form. Trades speed for nuance.
Mentalyc gives you access to all of these templates in one place, so you can switch formats per client or per payer without rebuilding your workflow. For a broader overview of every note type clinicians use, see our mental health notes overview.
Real-World Comparison: One Session, Three Formats
The same therapy session can be documented in very different ways depending on the format you choose. Below is how a single session looks in SOAP, DAP, and Narrative form.
Client: Age 25 with PTSD
Focus: Recurring nightmares and dissociation
SOAP
- S: Client reports three nightmares this week.
- O: Fatigued and fidgety.
- A: Signs of persistent hyperarousal.
- P: Continue EMDR; increase journaling.
DAP
- D: Client reported sleep disruptions and appeared withdrawn.
- A: Ongoing trauma-related symptoms.
- P: Review safety plan; continue EMDR.
Narrative
The client described waking disoriented from trauma-themed dreams and growing fearful of falling asleep. Therapist validated the experience and introduced grounding tools.
The format does not just change how you write. It changes how you think, plan, and track client progress. These are not stylistic preferences alone, they shape how your care is understood by supervisors, insurers, and your future self.
What to Consider When Choosing a Format
Four factors should drive the choice.
Clinical orientation and therapeutic style. Let your approach guide your progress note format. Cognitive-behavioral therapists may lean toward SOAP or GIRP. Narrative or psychodynamic therapists often prefer open-ended styles that align with how they conceptualize cases.
Client needs and treatment context. Working with clients in crisis? Consider BIRP or PIRP for their structure. Supporting long-term insight-oriented work? Narrative or DAP may give you the room you need. Match the format to what is clinically relevant, not just what is easy.
Practice or agency requirements. Some employers, supervisors, or insurance panels expect a specific format. Even in solo private practice, payer requirements or legal compliance may influence your choice.
Time efficiency and workflow. A format that is clinically thorough but inefficient becomes a drain. DAP is often praised for its simplicity. Tools like Mentalyc can speed up documentation across formats without compromising quality.
Adapting Your Format as You Grow
When starting out, SOAP or DAP is often the safest bet. Both are widely accepted, easy to learn, and provide a helpful structure.
As you gain experience, your note style may evolve with your caseload or preferred modalities. You might adopt Narrative notes for some clients, or shift to GIRP if you are doing short-term solution-focused work. That is fine, as long as you are consistent within each client’s chart. If you switch formats mid-treatment, make a quick note explaining why:
“Switching to GIRP format as of [date] to support short-term, goal-focused treatment plan.”
That clarity helps during audits and supports continuity of care over time.
One Size Does Not Always Fit All
Some clinicians use different formats depending on the session type or client. BIRP for structured agency sessions, DAP or Narrative when the work gets more exploratory. Consistency within each client’s record is what matters most. The goal is intentionality, picking a format that captures your work without bogging you down, rather than rigidity.
GIRP Note Template and Example for Goal-Oriented Therapy Notes
GIRP notes have four sections: Goal, Intervention, Response, Plan. GIRP centers each note on a stated therapeutic goal, which makes it useful for goal-focused therapy, coaching, and utilization review.
Goal. The client presents for therapy, wanting to work on several life stressors. The client presents for treatment due to several recent changes they are having trouble adjusting to. The client reports they just got married and started a new job. The changes are causing significant stress and exhaustion.
Intervention. The counselor will work with the client on developing three to five strategies for reducing and coping with stress. The counselor will allow the client space to discuss and process how stress is impacting them.
Response. The client states they “are happy to start therapy and work on stress management skills.” The client is attentive and focused in the therapy session.
Plan. The counselor will meet with the client bi-weekly to address stress management techniques. The client’s next session is Friday at 10 a.m.
PIRP Note Template and Example for Problem-Focused Progress Notes
PIRP notes have four sections: Problem, Intervention, Response, Plan. PIRP is organized around an identified clinical problem, which works well for crisis sessions and short-term work.
Problem. The client presents for therapy and states her problems include meth use and depression. The client reports, “meth use has ruined my relationships with others.” The client struggles to pay her bills and says she has been clean from methamphetamine for one week. The client would like to work on assistance with paying her bills and identifying additional recovery resources to help her continue abstaining from meth use.
Intervention. The therapist utilized motivational interviewing techniques to assess the client’s substance use history and readiness to change. The therapist helped the client explore triggers for using methamphetamines. The therapist gathered a history of the client’s depressive symptoms; the client reports being depressed for about two years, around the time methamphetamine use increased.
Response. The client appears to be in the action stage of change with their methamphetamine use. The client reports being motivated to stay clean and to learn more about depression and substance use.
Plan. The client will attend weekly therapy sessions with the therapist. The client will attend one NA group per week. The therapist will refer the client to a caseworker who can help address financial assistance resources.
For private practice owners and group practices managing high volume, Mentalyc’s AI Note Taker cuts documentation time so clinicians stay focused on clinical care.
Custom Format Mental Health Progress Note Template and Example
This format does not follow a single template but includes everything required for billing and insurance. Use it when your payer asks for specific sections such as risk assessment and presenting problem.
Mental status. The client presents with a euthymic mood. The client appears well-dressed and speaks at an average volume and pace. The client is oriented to person, place, and time.
Risk assessment. The client presents no significant risk of harming themselves or others.
Presenting problem. The therapist and client have been working to address communication problems in the client’s relationships with their partner and friends. They are working on using “I” statements.
Assessment. The client reports difficulty in their relationships before engaging in therapy. The therapist has been educating the client about healthy relationships in prior sessions. The client says they have been able to utilize “I statements” when bringing up difficult conversations with their partner.
Therapist intervention. The therapist provided the client with psychoeducation on healthy communication skills and introduced them to Gottman’s Four Horsemen of the Apocalypse.
Plan. The client is progressing in therapy and will probably need two more sessions to complete this work. The client will meet with the therapist next week and the following week, then terminate treatment.
Case Management Note Template and Example
Case managers work on client needs adjacent to mental health: housing, benefits, employment, transportation. The case management note template below structures that work without losing clinical relevance.
Problem. The client presents for case management services to work on finding housing and applying for food stamps. The client was able to obtain the paperwork but needs help filling it out. The client has been staying in a homeless shelter and would like to find their own place.
Treatment plan goal. The client will obtain housing and food assistance.
Intervention. In this session the case manager spent an hour assisting the client with applications for food stamps and low-income housing. The case manager educated the client on where to submit applications and provided transportation to the community service agency.
Client response. The client filled out their applications and expressed gratitude for the assistance of the case manager.
Plan. The case manager will meet with the client bi-weekly to track application progress and, if denied, help the client access other community resources.
CBT Note Template and Example Using SOAP Format
A CBT note can use any base format. Below is a CBT-informed session documented as a SOAP note.
Subjective. The client presents for therapy due to social anxiety. The client states they do not like leaving their house because they do not want to interact with people they do not know. They often have to lead meetings and give presentations at work, which makes them feel jittery. The client reports poor sleep quality and work difficulties due to social anxiety.
Objective. The client has an anxious presentation. They are talking rapidly during the session. The client appears nervous and anxious while speaking with the psychotherapist.
Assessment. The client has symptoms consistent with social anxiety disorder. The psychotherapist will monitor anxiety symptoms through the Liebowitz Social Anxiety Scale. The psychotherapist will work with the client utilizing CBT methods to identify and replace irrational thoughts. The psychotherapist will also help the client identify cognitive distortions and how these distortions affect their life.
Plan. The psychotherapist and client will meet weekly for therapy. The client will keep a CBT thought log of anxious thoughts to review in each session.
Couples Therapy Note Template and Example
Couples therapy notes focus on the dynamic between two people in a relationship rather than on one client’s symptoms. The example below documents a session focused on communication.
Presenting problem. The couple presents for therapy wanting to work on communication differences. The couple reports that when they try to communicate they often end up yelling at each other, which results in no teamwork to accomplish their goals or solve problems. They state that they both end up shutting down, which leads to an emotional disconnect. They want to work toward communicating better and finding ways to resolve conflict.
Themes and patterns identified. The social worker observed that the couple tends to sit far away from each other in session. They appear physically and emotionally disconnected. The couple has insight into their challenges with ineffective communication and report that the yelling and disrespectful communication increases when they are both stressed.
Discussion. The couple shuts down when they feel disrespected. They use stonewalling often to communicate a message, but this method drives them further apart as it does not resolve the issue. The “silent treatment” then begins to feel like a punishment to them both, and they never talk about the issue again.
Plan. The social worker addressed and provided education to the couple about Gottman’s Four Horsemen of the Apocalypse in session. The couple voiced understanding about what this means and were able to identify some examples of how this shows up in their relationship. The social worker will educate them on the antidotes to the four horsemen in the next session.
Homework. The couple was encouraged to write down any incidents of the four horsemen appearing in their day-to-day life before the next session.
PIE Note Template and Example for Mental Health Documentation
PIE notes have three short sections: Problem, Intervention, Evaluation. They work well for brief sessions and adolescents.
Problem. The adolescent presents for a therapy session with reports of falling behind in school. The client has always been a straight A student, but grades have worsened this year, which has been happening for about six months. The client reports an increase in the difficulty of schoolwork. They have trouble focusing at school and home and avoid homework because they find it challenging. The client states that when they are at school, the environment is “too loud to focus.”
Intervention. The counselor will work with the client on reducing symptoms of ADHD. The counselor will work with the client’s parents and school, with parental permission, to request accommodations. The counselor will educate the client on strategies to manage ADHD and provide psychoeducation to the client and parents on supporting tools.
Evaluation. The client’s symptoms are consistent with a diagnosis of ADHD. The client was receptive to this. The client and parents are on board with learning new strategies and working with the school.
Play Therapy Note Template and Example
Play therapy notes document how the child engaged in play and what interventions you used. Format varies; the example below covers the core elements.
Presenting problem. The child presents for therapy because the parents state the child throws more tantrums at home. The child is eight years old and in second grade. The parents report the child is doing well in school but at home is refusing to clean their room and throwing tantrums when asked to do something. The parents want the child to learn to manage emotions better.
Techniques. The psychologist will provide client-centered play therapy techniques with the child to work on better identifying and managing emotions. The psychologist utilized tracking and limit setting during this session to help the client identify emotions.
Response. The child was shy and reluctant to engage in play therapy at first. The client then played with the dollhouse for the majority of the session. The client preferred independent play and shut down when the psychologist talked about how the dolls might be feeling.
Plan. The psychologist will continue to meet with the child weekly for play therapy and continue to build trust and rapport.
Group Therapy Note Template and Example
Group therapy notes document what occurred in the group as a whole and how the individual responded to the facilitator and other members. The example below documents a substance use group.
Group focus. The group focus today was identifying triggers to substance use. Identifying triggers is key in relapse prevention and helps the group identify barriers to sobriety.
Client mood. The client presented with depressed mood.
Group facilitator interventions. The facilitator encouraged the group to identify triggers that lead them to use drugs. The facilitator encouraged sharing about triggers to help group members process them. The facilitator assisted group members with identifying how they could respond to triggers, make different choices, or avoid them altogether. The group members actively engaged in a discussion about avoidable and unavoidable triggers.
Individual response to group. The client responded well to the group discussion and shared about her triggers. She had to be prompted to engage at first, then became an active participant after some encouragement.
Plans and recommendations. The group facilitator recommends that the client continue to attend group sessions weekly. The facilitator also recommends that the client continue individual therapy sessions weekly to address depression.
Custom Format Progress Note Template with a Strengths Section
This format can be tailored to each clinician. The example below adds a strengths section, which many trauma-informed and humanistic practitioners include.
Presenting problem. The client presents for therapy, wanting to work on steps to come to terms with their sexuality. The client reports accepting parents but struggles with coming out to extended family for fear of judgment. The client has moderate anxiety and would like some strategies for dealing with it.
Mental status. The client presents with an anxious presentation. The therapist can sense that it is difficult for the client to attend therapy and discuss their sexuality.
Assessment. The client appears to have anxiety and seems nervous about discussing their sexuality in depth in the first session. The client will likely need to build trust and rapport with the therapist before digging into family history and coping.
Intervention. The therapist will educate the client on the stages of coming out. The therapist will first work to develop trust and rapport. When the client is more trusting, the therapist will use ACT techniques to help the client respond to coming out.
Strengths. The client can ask for help and has a strong support system consisting of friends and parents.
Areas to work on. The client is anxious and may have difficulty opening up initially.
Plan. The therapist and client will meet weekly.
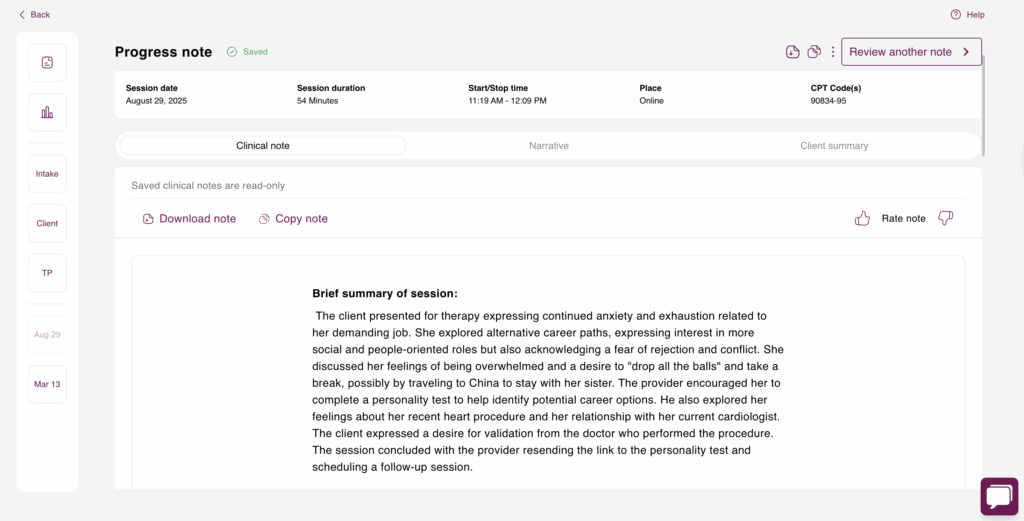
Mentalyc SOAP Note Example
This is what a Mentalyc-generated SOAP note looks like in practice. The format meets medical necessity requirements and uses evidence-backed interventions, which makes it easy to track client progress over time. Using Mentalyc for templated notes is a leading solution for improving therapist productivity.
Subjective.
The client presented for therapy reporting fluctuating emotions, work stress, and self-critical thoughts. She denied any self-harm. She described two instances of near emotional shutdown during the week. A review of her DBT diary card indicated moderate avoidance urges and distress (7/10) specifically related to a workplace conflict. The client’s work stress appears to be significantly impacting her emotional regulation and ability to manage conflict.
Objective.
The client’s presentation and concerns were assessed through a clinical interview and review of her DBT diary card. The diary card provided data on urges, skills utilization, and distress levels. Paced breathing and grounding techniques were utilized during the session. CBT work focused on restructuring the automatic thought, “I can’t handle this job,” using Socratic questioning to generate counter-evidence. This led to the reframed thought, “The job is demanding, but I have evidence that I can manage it,” with the client reporting a 65 percent belief in the new thought, up from 30 percent. Mindfulness practice was employed to help the client label her emotions (hurt, anxious, small) after she became tearful mid-session while recalling her supervisor’s tone, which triggered memories of childhood criticism. This intervention successfully reduced her distress level from 7/10 to 4/10. The session also explored the connection between her self-criticism, authority-triggered anxiety, and the core belief “I’m not good enough.”
Assessment.
The client actively engaged in the session and demonstrated a strong therapeutic alliance by openly sharing vulnerable emotions and experiences. She showed a positive response to both CBT and DBT interventions, successfully utilizing learned skills and demonstrating improved emotional regulation through mindfulness and thought reframing. While she presented with mild risk due to reported near emotional shutdown, her active engagement and willingness to utilize coping skills suggest a positive trajectory. Continued monitoring of her emotional distress remains important.
Plan.
The client’s homework includes daily paced breathing practice, particularly during work breaks; identifying and reframing automatic thoughts at least once per day; and continued use of the DBT diary card. Future sessions will focus on continuing CBT and DBT skill development to address work stress, self-criticism, and emotional regulation. Further exploration of the connection between current experiences and childhood experiences with a critical parent will be a focus of ongoing treatment.
Over time, tools like Mentalyc’s AI Progress Tracker turn this kind of documentation into a visual view of symptom reduction and treatment response, which is especially useful when justifying continued care to insurers.
Mentalyc AI Pricing Plans
| Plan | Price | Key features |
|---|---|---|
| 14-Day Free Trial | $0 | 14 days of full Pro access, including 15 notes. No credit card required. |
| Mini | USD 14.99 per month | Record in-person sessions, upload audio files, use voice-to-text, or type notes directly. |
| Basic | USD 29.99 per month | Everything in Mini, plus Alliance Genie (limited access) and AI Treatment Planner. |
| Pro | USD 59.99 per month | EMDR, Play and Psychiatry modalities, 100+ custom templates including BIRP, PIRP, GIRP, PIE, and SIRP, auto-computed CPT codes. |
| Super | USD 99.99 per month | Everything in Pro, plus group therapy notes for each group member and priority onboarding and support. |
For more details, visit the pricing page.
Mentalyc DAP Note Example
This is what an AI-generated DAP note looks like for the same kind of session. It is concise and clearly shows the client’s progress and the therapist’s actions.
Data.
The client presented with significant anxiety (8/10) primarily related to work and health concerns, which impacted her sleep and social interactions. She reported avoiding phone calls due to low energy. Her anxiety manifests as racing thoughts, difficulty sleeping, and avoidance of social interaction, significantly impacting her ability to connect with friends. The client’s current high anxiety levels have persisted over the past few days, escalating particularly at night.
Assessment.
A clinical interview was used to assess the client’s anxiety, triggers, and treatment effectiveness. The client actively engaged in the session and responded positively to the interventions. She demonstrated a willingness to practice coping skills and experienced a reduction in anxiety from 8/10 to 5/10 by the session’s end. She successfully formulated an alternative statement to challenge catastrophic thoughts and expressed motivation to continue practicing the discussed skills. However, the client also reported struggling with intrusive thoughts during mindfulness exercises, presenting a potential challenge to her continued practice. Due to her high anxiety and social withdrawal, she is considered to be at mild risk, necessitating continued monitoring.
Plan.
The client’s homework includes continuing mindfulness practice, particularly at night before bed. She is to practice reframing catastrophic thoughts when physical anxiety symptoms arise. She is also tasked with attempting one social connection, either by answering a call or initiating a brief check-in with a friend. Future sessions will focus on continuing work with CBT and DBT skills to manage anxiety and promote social engagement, as well as exploring any ongoing challenges with mindfulness practice. Continued weekly therapy sessions are planned to integrate CBT and DBT skills to manage anxiety, improve emotional regulation, and address avoidance behaviors.
Write audit-ready notes in minutes, not hours
- Generates specific, measurable, audit-ready language
- Never skips a required section
- Locks in one consistent template per client
- Writes a fresh Assessment every session

Common Mistakes to Avoid in Progress Notes
Knowing what to do is half of it. Knowing what to avoid is the other half. Six failure modes show up most often in audits and peer reviews.
1. Lack of clarity. Vague summaries like “client seemed better today” tell a reviewer nothing. Replace with specific, measurable language: “Client maintained eye contact 80 percent of the session and reported sleeping 7 hours a night for two consecutive nights, up 4 hours from last week.”
A second worked example: “The client described having 3 episodes of panic attacks this week. This has reduced from 5 last week. Each attack lasted about 15 minutes. The attacks presented with rapid breathing, chest tightness, and racing thoughts. The client was encouraged to continue using grounding techniques and monitor the symptoms.”
One practical fix is to write the unclear note in BIRP format – [B]ehavior (what you observe), [I]ntervention (therapeutic approach), [R]esponse (of clients), and [P]lan. Forcing each section makes ambiguity hard to leave in. Example: “Client practiced 10 minutes of deep breathing exercises in today’s session. Anxiety levels reduced from 8/10 to 4/10 on the subjective units of distress scale. The client was advised to continue deep breathing exercises daily and track the anxiety levels for review in the next session.”
2. Incomplete information. Missing the client’s current mood, the intervention used, the client’s response, the updated risk assessment, or changes to medication breaks continuity of care and can delay treatment.
3. Inconsistency across documentation. Switching note formats mid-treatment, using different wording for the same condition, or alternating between detailed and brief notes makes progress impossible to track. Standardize abbreviations, terminology, and templates.
4. Errors in the Subjective section. Listing personal interpretations as if the client said them, recording irrelevant detail, or ignoring significant mood or behavior changes. Record the client’s own words, link statements to observable behavior, and avoid judgments.
Worked pair:
Incorrect: The client displayed signs of depression together with a lack of motivation.
Correct: The client reported feeling moody most days. He also found it difficult to get up from his bed. He started sleeping 12 hours daily and missed work twice this week.
The client’s current state should be clear in subjective documentation while professional boundaries and clinical relevance are preserved. That balance is what lets the Subjective section actually show progress and detect patterns over time.
5. Assessment redundancy. Copy-pasting outdated assessments across sessions, or restating what is already in Subjective or Objective. Focus the Assessment on new developments, link observations to treatment objectives, and document the reasoning behind interventions.
Strengthen the Assessment with specific examples rather than general statements. Weak: “Client is doing better.” Strong: “Client shows improved emotional regulation. He uses deep breathing techniques when faced with anxiety triggers.” Distinguish between persistent concerns and new developments. The Assessment should combine present and past information to show current condition AND therapeutic progress, not just restate the file.
6. Vague plans. “Continue therapy” or “apply CBT techniques” is not a plan. Specify the intervention (“use thought-recording worksheets”), make goals measurable (“reduce panic attacks from 3 per week to 1 per week within 30 days”), and include the next appointment date.
Worked pairs:
Weak intervention: “Apply CBT techniques.” Strong: “Use thought-recording exercises and provided worksheets.”
Weak goal: “Reduce anxiety.” Strong: “Decrease panic attacks from 3 times a week to once a week within 30 days.”
The timeline aspect should include the next date of appointment, frequency of sessions, expected milestone dates, and review periods. Maintain a direct connection between plan, assessment, and client objectives.
A useful frame for the Plan section: every plan element should be SMART. Specific, Measurable, Achievable, Relevant, Time-bound.
Mentalyc’s AI Note Taker was built to solve mistakes 1, 2, 3, and 5 directly. It generates specific, measurable language from the actual session content, will not skip required sections, locks in a consistent template per client, and writes a fresh Assessment each time rather than copy-pasting prior ones.
Make Progress Notes Easier with Mentalyc
To cut documentation time without losing audit-readiness, sign up for Mentalyc. The AI Note Taker records or ingests your session and drafts a SOAP, DAP, BIRP, GIRP, or PIRP note in about two minutes. See real Mentalyc note examples across every format if you want to compare the output before signing up. The AI Treatment Planner keeps interventions aligned with measurable treatment plan goals so medical necessity is visible in every note. The AI Progress Tracker turns your notes into a visual view of symptom reduction over time, which holds up well in payer reviews.
For visual walkthroughs of how to structure progress notes using different templates, see Mentalyc’s YouTube channel.
Watch Real Stories from Mentalyc Users
Frequently Asked Questions About Mental Health Progress Note Templates
Why other mental health professionals love Mentalyc

“I really like that the treatment plans make sense, and they’re based on the case notes I’ve been entering.”
Therapist

“The treatment plan gives me a place to look with clients and say, here’s where we are and here’s where we’re aiming to go. It’s such a huge help.”
LPC

“Do yourself a favor, make your life easier. I found Mentalyc to be one of the best tools that I’ve ever used.”
Licensed Marriage and Family Therapist

“For anyone hesitant: this is a lifesaver. It will change your life, and you have more time to be present with your patients.”
Licensed Clinical Social Worker
References
1. Centers for Medicare and Medicaid Services. Medicare Benefit Policy Manual, Chapter 15: Covered Medical and Other Health Services. Section 80.2 (Outpatient Mental Health Services). Documentation timing guidance: complete within 72 hours of service.
2. Centers for Medicare and Medicaid Services. Documentation requirements for outpatient psychotherapy services. Notes must support medical necessity by documenting diagnosis, interventions, client response, and progress toward treatment goals.
3. American Psychological Association. Record Keeping Guidelines. Guidance on structure, length, and content of psychotherapy records.
4. Health Insurance Portability and Accountability Act of 1996 (HIPAA), 45 CFR section 164.501. Definition of psychotherapy notes and the protections distinguishing them from the general medical record.